

Let’s Get It Clear: Measurements in seating – Relative angles in a seating system

Last month we looked at what we need to do to measure the angles between different parts of the body with respect to the needs of a seated person. This month we review how these angles ultimately relate to a person’s seating system. There are important aspects that ensure that the seating system prescription meets the seated person’s needs. The key take-home message is that the body’s relative angles frequently do not equate to those of the seating system, or vice versa.
A standard was published in 2006 (ISO 16840-1)1 which for the first time introduced a standardised means of measuring a seated person and their seating system in a wheelchair. This is important so that one assessor’s measures are similar to the next assessor’s Inevitably the language of standards is not always an easy read, and so Kelly Waugh and Barbara Crane produced a Clinical Application Guide (CAG) which is available for free download2 – giving greater in-depth coverage of the material summarised here.
In the previous article we looked at the relative angles of the seated person, while in this article we concentrate on the relative angles of their seating system.
First principles
Relative support surface angles are usually taken from the side view, the ‘sagittal’ view. Relative angles of support surfaces in the frontal and transverse planes are rarely used in practice.
All relative angles are measured from the occupant side of one support surface to the occupant side of the adjacent support surface, with the surfaces unloaded.
Any angle can be measured on two sides (one side less than 180 degrees and the other greater than 180 degrees). The side of the angle which is used is based on clinical intuitiveness, with a preference for using the angle which gives a smaller value when the surfaces are oriented in a ‘neutral’ seating position.
The three primary support surface relative angles – seat to back support angle, seat to lower leg support angle, and lower leg support to foot support angle – are the most commonly specified support surface angles in practice, because deviations in these angles will have the most profound effect on seated posture.
Locating the relevant support surfaces
Relative support surface angles are defined as the angle between two adjacent support surfaces, and so you need to be able to locate the relevant parts of the two adjacent support surfaces in order to align your goniometer arms. If the contact surface side of the body support device is flat, you can lay the arms of the goniometer or angle finder directly on the contact surface itself, or parallel to the flat contact surface side of the support.
For contoured seat or back support surfaces, this is more difficult. There are two ways to identify the relevant part of the support surface when the surface is contoured:
- Use the solid, flat structure on the non-contact surface side of the support: The support surface lines of a contoured seat or back support cushion can be approximated using the flat pan or shell on the non-contact surface side of the seat or back support device.
- Use a clipboard or other flat surface placed onto the contoured contact surface.
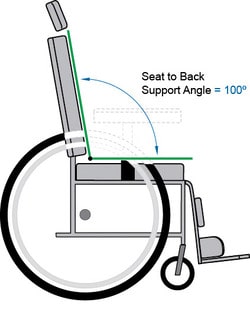
Example – Seat to back support angle
The most common relative angle of the seated person is the thigh to trunk angle, and this angle of the seating system relates to this body angle, but frequently is not the same value, and ideally is measured with the occupant in place in the seating system at the required thigh to trunk angle, and then the angle of the seating system to achieve this can be measured.
The clinical relevance is that the angle between the seat and back support can have a significant influence on the individual’s comfort, posture, health, and function, and therefore it can be clinically useful to document the existing and/or desired seat to back support angle.
SEAT TO BACK SUPPORT ANGLE
Type of Measurement:
Relative support surface angle
Description:
The angle between the seat and the back support viewed from the side.
Surfaces used:
- Back support surface
- Seat cushion surface
Angle measured:
The anterior side of the angle formed between the back support reference plane and the seat reference plane, as viewed from the side.
Typical Values:
80 -120o
Sample Procedure (using a goniometer):
- Locate the seat and back support surfaces
a) If the seat and/or back support surface is flat, align the arms of the goniometer along or parallel with the flat contact surface side of the seat and of the back support cushion.
b) If the seat and/or back support surface is contoured, their surfaces can be approximated using the flat pan or shell on the non-contact surface side of the seat or back cushions. In this situation, align the arms of the goniometer along or parallel to the flat solid backings behind the back support cushion and under the seat cushion to approximate the seat to back support angle. Alternatively, place a clipboard or other firm flat surface on top of the contact surface to approximate the surface.
- Measure the angle
a) Align the stationary arm of the goniometer along or parallel to the back support surface.
b) Align the moveable arm of the goniometer along or parallel to the seat cushion surface.
c) Read the internal, anterior side of the angle.
Considerations
- This measure is used when there is a single continuous back support surface. If the back support is sectioned, as in a bi-angular back support, you may wish to measure both the seat to lower back support and the seat to upper back support angles.
- The seat to back support angle is very critical as it can influence the user’s posture and function in many ways. This relative angle is typically chosen to support the person’s body at the desired thigh to trunk angle, which is unique to that individual. The desired thigh to trunk angle is typically based on the user’s hip joint flexibility, level of postural control of the trunk, presence of muscle spasticity, and functional needs with respect to orientation of the trunk, head and upper extremities.
- If the seated person’s trunk is parallel with the back support reference plane, and their thigh is parallel to the seat reference plane, then the seat to back support angle will be the same as the person’s thigh to trunk angle.
Lower leg measures
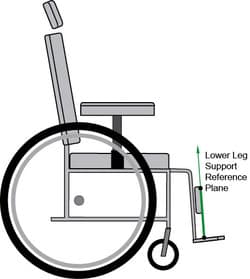
The lower leg support surface can be difficult to identify because frequently there is not an actual lower leg support device, such as a ‘calf pad’, on the wheelchair. However, this ‘surface’ is necessary for measuring the seat to lower leg support angle and the lower leg support to foot support angle.
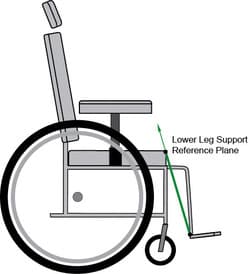
There are two ways to identify the lower leg support ‘surface’, based on whether there is a posterior lower leg support device on the system being measured, and these are summarised in Figure 2. The lower leg support ‘surface’ can be an imaginary line intersecting the rear edge of the foot supports or heel loops and the most forward projection of the seat.
Where there is a lower leg support device, such as a calf pad, on the wheelchair, the lower leg support surface is defined by the contact surface of the posterior lower leg support at its geometric centre. Note that this lower leg support line may project forward of the end of the seat cushion, and the bottom may not project to the back of the foot support; however the posterior lower leg support line will be defined by the orientation of this pad.
This makes sense clinically, because the location and orientation of a calf pad will affect the person’s lower leg alignment.
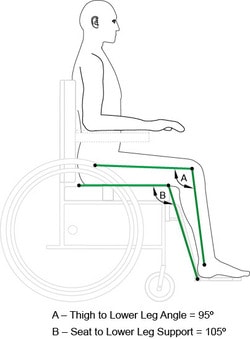
Seat to lower leg support angle
This angle is generally prescribed to match the desired thigh to lower leg angle of the person, which is based on the user’s hamstring flexibility, knee joint range of motion, comfort and stability needs, as well as other functional considerations such as manoeuvrability of the mobility base.
The most common way to alter the seat to lower leg support angle is to change the anterior-posterior position of the foot support relative to the front edge of the seat.
This angle generates a significant amount of confusion among clinicians and suppliers, yet it is a critical dimension to specify and therefore it is important to communicate information about this dimension accurately.
The seat to lower leg support angle is a support surface angle, not a body segment angle. Specification of this angle is used to achieve a certain thigh to lower leg angle, however they are often not exactly the same value. This is because the centre of the user’s knee is forward of the end of the seat, and therefore the centre point, or vertex, of the body segment angle and the support surface angle do not line up.
For example, if a user’s knee is several inches forward of the end of the seat (in a system with no posterior lower leg support), the user’s thigh to lower leg angle will be significantly less than the seat to lower leg support angle (Fig. 3). Additionally, if the back of the user’s foot is not positioned at the back of the footplate, there will be a greater discrepancy between these two angles.
Lower leg support assembly angle is something else
The lower leg support assembly angle is a wheelchair frame angle, and not a seating support surface angle, and it is defined and measured very differently. The 60-70-90 degree angle of the lower leg support assembly of the wheelchair frame, used by manufacturers, refers to the angle formed between the forward projection of the seat rail and the leg support hanger tube.
Not only is the value determined differently, but it also represents the orientation of frame components and not necessarily the orientation of seating support surface components mounted onto the wheelchair frame. The wheelchair’s lower leg support assembly angle is typically fixed, and does not change with varied placements of the seat or foot supports. Conversely, changes in the position and/or angle of the seat cushion or foot support will change the seat to lower leg support angle.
References
- ISO 16840-1:2006 Wheelchair Seating, Part 1 – Vocabulary, reference axis convention and measures for body posture and postural support surfaces
- Waugh, K and Crane, B (2013) A clinical application guide to standardized wheelchair seating measures of the body and seating support surfaces. Accessible as BPG3 from www.pmguk.co.uk/resources/best-practice-guidelines/bpg-archive
Further items can be found at www.beshealthcare.net. If you are interested in receiving further information on the topic, please contact  barend@beshealthcare.net.
barend@beshealthcare.net.
Dr Barend ter Haar has been involved in seating and mobility for over 30 years, including lecturing internationally and developing international seating standards.
