

Let’s Get it Clear: What makes a good positioning belt? Safety first

In previous issues of THIIS in the Let’s Get it Clear series1, we have covered various aspects of ‘What makes a good positioning belt?’. The previous articles in this series covered the anatomy of a pelvic positioning belt; hoosing and adjusting a pelvic positioning belt; the features and benefits of different belt closures; means to fix the belts to the wheelchair frame in appropriate positions; and selection of anterior harnesses to optimise the position of the trunk.
Positioning belts and harnesses are provided primarily, as the name suggests, for the purpose of positioning. They are not ‘safety belts’ in the way that vehicular occupant restraints are also named, in that those devices are to protect the person from being thrown forward in a car accident.
However, it is important that the occupant of a seating system is safe. The safety elements include avoiding failure of the postural support device (PSD), avoiding slippage of the PSD, avoiding skin tissue damage arising from pressures from the PSD when tightened, avoiding asphyxiation, and avoiding falling out of the seat.
There have been recorded injuries and deaths resulting from inappropriately placed or adjusted positioning belts and harnesses, leading to both falls and strangulation. It was for this reason that BS 8625 was published in the UK in 2019, and now adopted internationally in ISO/TS 16840-15 (due for publication this year, 2022), to cover the ‘Selection, placement, and fixation of flexible postural support devices in seating’. In these standards, guidance is given for safe practice, and requirements that secondary supports are tested to ISO 16840-32 and ISO 16840-103.

Pelvic positioning
Some of the deaths have occurred as a result of occupants ‘submarining’ under their pelvic positioning belts. To avoid the risk of ‘submarining’, it is critical that the belts are not fitted at the junction between the back support and the seat structure – this 45 degree angle is appropriate for a vehicular occupant restraint belt, but not for a positioning belt.
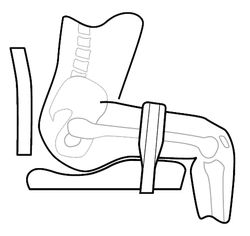
For those clients at risk of going into posterior pelvic tilt and, as a result, of sliding forward in their seat, the standards cited above require that the belt is positioned anterior to the greater trochanters (Figure 1).
The shorter length of belt material involved in positioning the pelvis means that the pelvis would not be able to slip under the belt (as long as it is tightened appropriately). In addition, this positioning in front of the greater trochanters means the occupant is able to reach much further forward, and there’s less pull down on the pelvis, and thus decreasing pressures on the ischial tuberosities.
Interestingly, in a paper presented at the recent European Seating Symposium meeting, Van der Heyden and Siefert showed that the shear forces through the skin tissues are very high when the belt is at 45 degrees, whereas at the preferred position they are minimal. Greater skin health all round and a much safer positioning solution!
Sources of asphyxiation (see Annex E of BS 8625 AND ISO/TS 16840-15)
Asphyxiation can arise from the use of postural supports for one of the following reasons:
- The support is too high and it occludes the airway (strangulation). This could be because:
- the support has been fitted too high; or
- the support has been adjusted since fitting to sit too high; or
- the support has moved out of position since being fitted.
- The occupant collapses down in the seat and the airway is occluded by the support. This could be because:

Figure 1: Options for correct positioning of a pelvic positioning belt (ISO/TS 16840-15)
- there is insufficient lateral trunk support such that the occupant collapses to one side; or
- there is insufficient posterior pelvic or lumbar-thoracic support to maintain an upright posture, such that the occupant collapses down into kyphosis.
- The occupant slides down in the seat and the airway is occluded by the support. This could be because the postural support is:
- fitted too loosely;
- poorly positioned; or
- malfunctioning.
- Mechanical compression is otherwise applied to the neck, ribcage, and/or diaphragm, due to:
- the anterior support strap/pad being fitted too tightly;
- the occupant sliding underneath the postural support until stopped by their arms and ribcage, placing pressure on the ribcage; or
- the occupant submarining totally underneath a postural support until they are stopped by the support being caught around their neck.
Protection against asphyxiation
Use of an anterior trunk support comes with an increased risk of injury or death due to asphyxiation/strangulation – this is greater when a chest support is used, as compared with a shoulder harness, due to the neck shape integral to the design of the support.
Any anterior trunk support should be supportive, but not restrict the physiological functions ongoing within the torso, whether this be digestive, respiratory, cardiovascular, or bladder function – and protecting all these internal functional requirements needs to be balanced with facilitating external physical functional needs. Furthermore, the risk is increased where the occupant is unable to recognise that something is incorrect about their seating, or cannot verbally express their distress.
- The first aspect of importance is that an anterior trunk support should never be used without a correctly fitted and adjusted pelvic positioning belt, to control the risk of ‘submarining’ under the pelvic belt (see Part 2 in this series, and BS 8625 for further guidance).
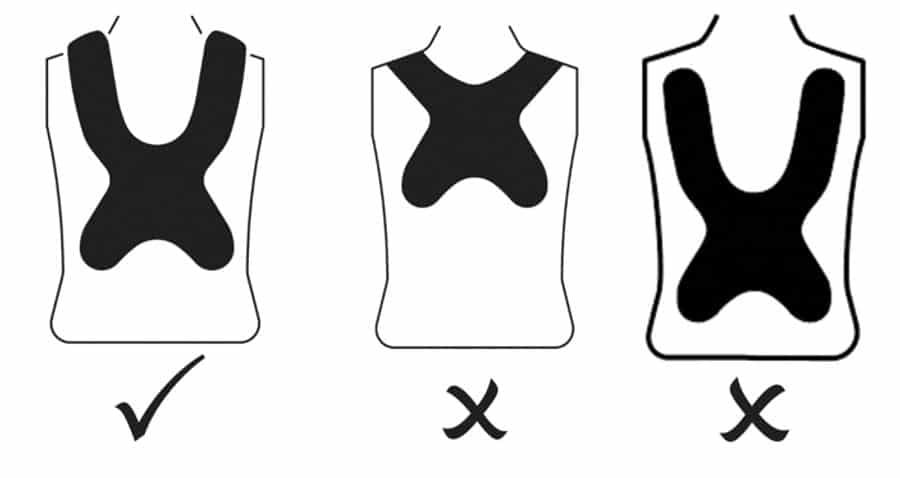
- The next aspect is that the central part of the support should be positioned no higher than the lower part of the sternum. ISO/TS 16840-15 provides the graphics (see Figure 2) for a label to be placed, if possible on the PSD, as well as in the IFU.
- The materials from which a chest harness is made is important. In consideration above of the dynamic elements built into a harness, the elasticity needs to be in the straps, and not in the central pad. Chest harnesses that are completely elastic, including across the central pad (sometimes referred to as butterfly harnesses), have a tendency to ride up and there have been reports of occupants being strangulated as a result.
Flexible PSDs should never be used as vehicular occupant restraints. They are by definition designed for postural positioning purposes, and their placement on a wheelchair, and their strength, for these purposes are very different from what is required from a vehicle’s safety belt.
In conclusion
A correctly fitted and fastened positioning belt or harness will enhance the occupant’s postural support, improving functionality and aiding good health. When done incorrectly, this can lead to harm or death. Do no harm, and follow the guidance and specifications in the standards.
References
1 https://thiis.co.uk/lets-get-it-clear-addressingmobility-and-posture-myths/
2 ISO 16840-3 Wheelchair seating – Part 3: Determination of static, impact and repetitive load strengths for postural support devices
3 ISO 16840-10:2021 Wheelchair seating – Part 10: Resistance to ignition of postural support devices – Requirements and test method
Further items can be found at www.beshealthcare.net. If you are interested in receiving further information on the topic, please contact  barend@beshealthcare.net.
barend@beshealthcare.net.
Dr Barend ter Haar has been involved in seating and mobility for over 30 years, including lecturing internationally and developing international seating standards.
Click to read more from the ‘Let’s get it clear’ series from Dr Barend ter Haar
