

Let’s get it clear: Restraint, rest, or support?

Different attachments around the body or around the mobility device have mixed use of terminology and confusion therein in their purpose, and as a result their application. The term ‘restraint’ has negative connotations, but there are many places where restraints confer a benefit to the client. This article reflects on where and when the terms ‘Rest’ or ‘Support’ may be more appropriate, and where ‘Restraints’ are relevant.
Restraint, rest, or support? When should we use which and where? Let’s start with perhaps the easier part: rest versus support.head supp
Rest vs support
On a chair, people still talk about back rests, armrests, and so on. Ever since ISO 7176 part 26 was published in 20071, the term ‘rest’ has been deprecated, and the preferred terms have been back support, arm support, etc. The term ‘support’ has connotations of the device providing an active function, whereas ‘rest’ implies passivity. The support element of these devices is to help position a person into a more functional posture, whilst also coincidentally increasing the weight-bearing surface area and thus potentially reducing the risks of tissue injury in the buttocks and sacral area.
The term ‘support’ thus has subliminal implications of improving function and other potential benefits and therefore, when this term is used, a more appropriate solution is more likely to be offered to the client.

A simple canvas-backed wheelchair is only offering, at best, a rest behind the client, and is generally only providing a means to stop the client falling backwards out of the chair (Figure 1). We spend time selecting an appropriate cushion to cover the client’s needs under their thighs and buttocks, to place on top of the canvas base, but often ignore the support that the trunk needs from an appropriately prescribed back support.
As we have covered in other articles in this series, the trunk has a vital role around many of our physiological functions, such as breathing, digestion, bladder control, etc. Proper support for the spine leads to a better posture – not only for these functions, but to get our heads into the optimal position for seeing, hearing, eating, and breathing. So let’s get away from the dis-service offered by a canvas-backed chair (unless for temporary use for transfer from say a house to a vehicle) and replace it by a proper back support!
Considering the arm supports for a moment: they may provide a degree of lateral support to the body and thus the distance from the trunk on either side will be of importance, and will in most cases be prescribed by the ‘width’ of the chair, or v.v.
For arm supports to provide appropriate support, their height is extremely important: too high, and the client’s arms will stick out too far to the sides of the chair, and the client will be uncomfortable – and may lose some degree of functionality for eating or other instances where they need their hands. Too low, and not only will the client slip down into a lordotic spinal curve, but also there will be less opportunity for weight redistribution under the arms. Therefore, adjustable height supports should be prescribed.
Head support?
The one area where any one of the three terms may be appropriate, is the device above the back support and behind the head.
- It is a ‘restraint’ where provided, on the likes of a powerchair, to stop the head from being thrown back too far during rapid deceleration – in the same way that we have head restraints on our car seats.
- It is a ‘rest’ where it is provided to catch the head when the seat is tilted back.
- It is a ‘support’ where it is used to help to position the head – either as a head support or a neck support.
The average adult head weighs about six kilograms and depends on its neck muscles to keep it upright and steady. As the day progresses and fatigue sets in, sub-occipital support behind the head, as a minimum, can help keep the head in position. For those who need more help, an extra lateral or anterolateral pad near the top of the head may help to provide a third point of control (Figure 2). (Just a word of warning – where a head support is used, ensure the client has a welladjusted pelvic positioning belt and anterior trunk harness in place to stop the client ‘hanging’ off the head supports.)

Positioning belts and harnesses
Positioning belts and harnesses bring us to the area where the most concerns tend to be expressed as to whether they are restraints. Restraint is a term that has different meanings and connotations, depending on the context of use. For this reason, RESNA produced a position paper2 to clarify the issue, in which the differences between supports and restraints are covered, as well as vehicular occupant restraints, and protective restraints.
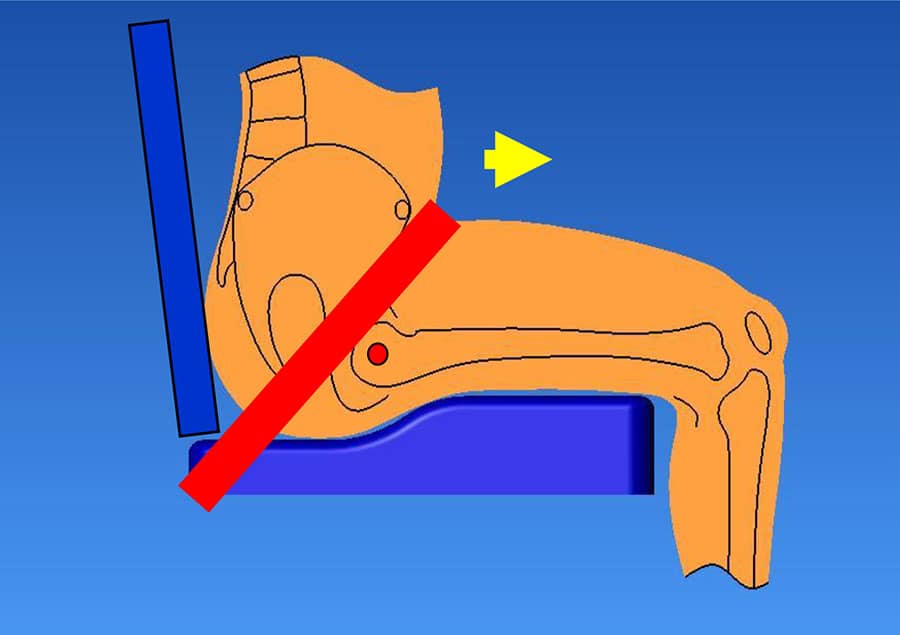
The first area to clarify is the difference between vehicular safety belts and postural management devices. The seat belts in your car or aircraft seats are there as restraints, so that in the ‘unlikely’ event of an accident, you are restrained in your seat, and not ending up head-butting the windscreen as the vehicle decelerates more quickly than your body. In summary: Wheelchair occupant restraint belts are generic devices which are used to restrain a wheelchair occupant in the event of a vehicular collision (Figure 3).
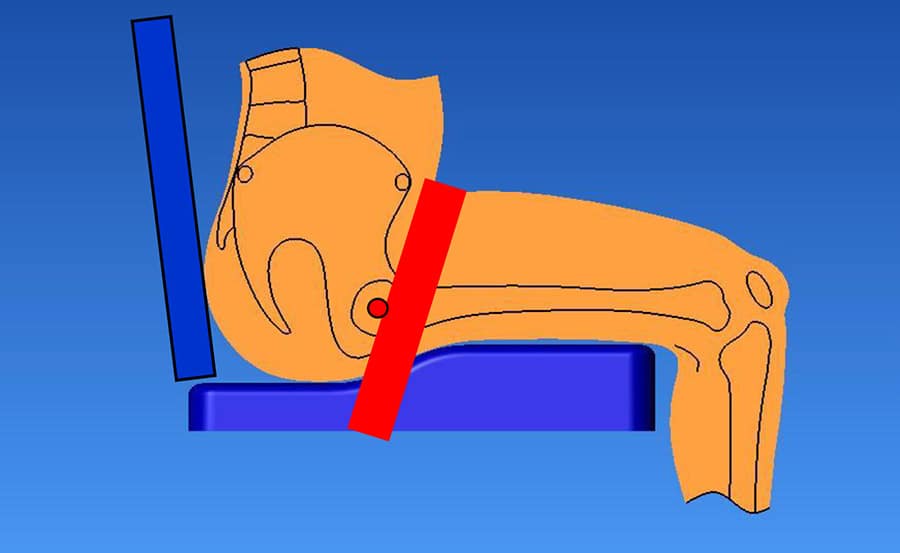
Wheelchair postural supports support a person’s posture, or position in their wheelchair. These supports are not intended to be used for, nor do they have the required strength to be used as, occupant restraints during vehicle transport (Figure 4).
Positioning supports shall not be used with the primary purpose of restraint. The topic is covered more extensively in BS 86253. In this standard it points out: “If a pelvic positioning support could be perceived as a restraint, the decision
to use the support shall be made by an interdisciplinary team, including carers, with the justification documented. The justification shall show that appropriate thought was given to alternative interventions, including, but not limited to, contracture management, tone management, and therapeutic intervention to address behavioural issues. Decisions shall, where practicable, be taken with the consent of the occupant, in the best interests of the occupant to ensure safety and function.
Any desired outcome resulting from the limitation of movement shall also be documented (e.g. to minimise the risk of falls). It shall also be documented where there is an aim to restrict movement in one part of the body, in order to facilitate greater function in another (e.g. fixation of the pelvis to improve postural stability).
Related to this topic could be the choice of buckle on a pelvic positioning belt. Depending on the client’s physical and/or their cognitive abilities, the ease of operation of the buckle comes into play – some are designed for easy release, but might therefore allow premature opening, while others may be more ‘fiddle-proof’, but might be more of a challenge for release in an emergency (see Annex C in BS 8625).
In the RESNA document, the concept of ‘protective’ restraints is also covered: there are times when some degree of restraint may be appropriate to protect the client from harming themselves (e.g. as a result of uncontrolled movements) or their carers around them.
References
- ISO 7176-26:2007, Wheelchairs – Part 26: Vocabulary.
- REHABILITATION ENGINEERING AND ASSISTIVE TECHNOLOGY SOCIETY OF NORTH AMERICA. RESNA Position on the application of wheelchairs, seating systems, and secondary supports for positioning vs restraint. RESNA: 2013.
- BS 8625:2019, Selection, placement and fixation of flexible postural support devices in seating – Specification.

Further items can be found at www.beshealthcare.net. If you are interested in receiving further information on the topic, please contact barend@beshealthcare.net.
Dr Barend ter Haar has been involved in seating and mobility for over 30 years, including lecturing internationally and developing international seating standards.
Click to read more from the ‘Let’s get it clear’ series from Dr Barend ter Haar
https://thiis.co.uk/lets-get-it-clear-restraint-rest-or-support/https://thiis.co.uk/wp-content/uploads/2021/10/image002.jpghttps://thiis.co.uk/wp-content/uploads/2021/10/image002-150x150.jpgAnalysis & InsightsLet's Get It ClearNewsroomarm support,armrests,back support,backrests,BES Healthcare,Dr Barend ter Haar,head support,Let's get it clear,RESNADifferent attachments around the body or around the mobility device have mixed use of terminology and confusion therein in their purpose, and as a result their application. The term ‘restraint’ has negative connotations, but there are many places where restraints confer a benefit to the client. This article reflects...Sarah SarsbySarah Sarsbysarah@thiis.co.ukEditorTHIIS Magazine