

Let’s get it clear: Asymmetry – The Good, the Bad and the Ugly

The textbooks like to show us as sitting in symmetrical positions, but in reality, we are all asymmetrical and we spend most of our time sitting asymmetrically. This article reflects on the benefits vs challenges of asymmetry and how we might manage the asymmetries in setting up a wheelchair seating system. We touch on belt and harness, lateral support pad, back support, headrest and even joystick positioning.
None of us is symmetrical – our left side is different from the right. Our heart is usually left of centre. Men are asked by tailors “do you dress to the left, sir?” Most of us have one foot larger than the other. We usually part our hair to one side. And so on.
Asymmetry is a fact of life, so why do we set up wheelchairs with the postural support devices in symmetrical positions for dealing with asymmetrical challenges? Probably because that is how the chairs are delivered from the factory.
The key thing here is to break the mindset that a belt, harness or other postural support device has to be mounted symmetrically. This article considers what the desired outcomes are and challenges conventional symmetrical positioning in achieving some of those outcomes.


Lower body
Starting at the pelvis, almost all pelvic positioning belts are mounted symmetrically i.e. the mounting points on the seat rails are each the same distance from the back of the chair to create a straight line across the occupant’s lap. Whilst this might be fine for many users, there are scenarios where it isn’t. For example, a client with a pelvic ‘windswept’ asymmetry in their posture might find that mounting the belt with offset mounting points can actually help correct or accommodate the asymmetry better.
Starting with the guidance to be found in BS 86251 that indicates when managing a tendency towards a posterior tilt, the belt should be mounted onto the seat rail anterior to the greater trochanters. This means that either side of the belt can still be mounted any required distance along the seat rail, anterior to the position of the greater trochanter on that side. A belt with a swivel buckle could be the best choice here to help with handling the forces around the buckle from the asymmetry, or the use of leg harnesses where there is a different strap attached to either leg (Figure 1), bespoke to the needs of that side of the pelvis.
Another asymmetrical challenge for clients with ‘rotation’ of the pelvis is that this frequently presents in combination with a pelvic obliquity, with the upper ‘forward’ part of the pelvis in anterior pelvic tilt and the lower ‘posterior’ side in posterior tilt. BS 8625 would suggest the former be addressed with a 4-point belt and the latter with a 2-point belt. The answer is to remove one narrow strap from your 4-point belt, to convert it into a 3-point belt: on the forward raised side of the pelvis, have the wider part of the belt pulling back against the ASIS on that side and fix that part of the belt to the back support uprights.
Have the narrower strap at right angles to come down in front of that side’s greater trochanter to stop the wider strap from riding up. On the side with the removed narrow strap, attach the remaining strap to the seat rail in front of that side’s greater trochanter. Voilà! We have an asymmetrical posture managed by an asymmetric belt set up (Figure 2).
Some clients, e.g. affected by a stroke, who wish to propel their wheelchair with their feet can only use one leg. For this asymmetry, the cushion may need to be set up to allow the active foot to be able to reach the floor, while the other leg needs to be fully supported along the thigh while that side’s foot is placed on a single foot support. A simple route to achieving this is to place a simple firm foam wedge (that is half the width of the cushion) under the part of the cushion on the side supporting the non-propelling leg (Figure 3).

Upper body
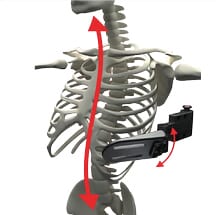
Moving up the body, in the article ‘Trunk call: Aligning the upper body’, I covered the importance of the positioning of lateral trunk supports for managing a scoliotic spine. Where the scoliosis occurs around the thoracic vertebrae, this can be managed by using the rib attached to the peak of the scoliotic curve as a lever to push the relevant vertebra. Please do take care that the support pad is not only pushing on the correct rib but also that the pad is rotated so that it pushes along the rib towards the vertebra (and is not a vertical pad which would displace the rib even further) (Figure 4).
The pads on the other side of the torso will be placed at different heights to the active side: active lateral trunk supports being used to handle a scoliotic spine will be asymmetric.
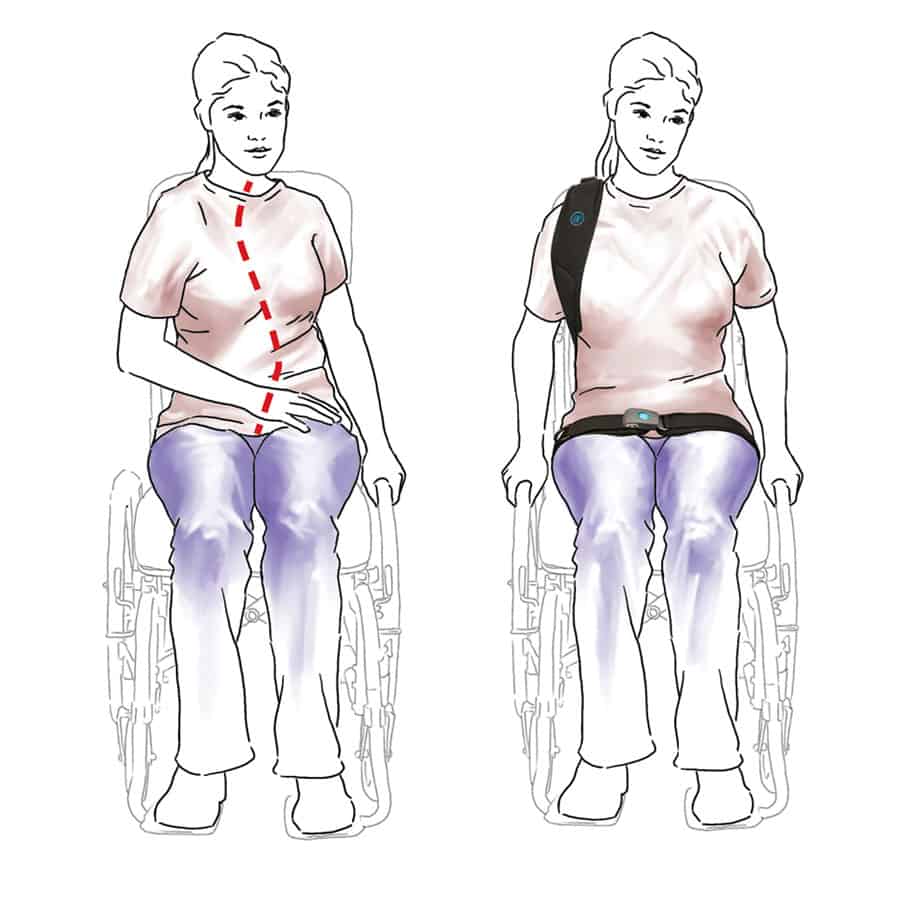
While managing a scoliotic spine, also consider where the back support shell is placed: if the spine is ‘off centre’ from the pelvis, select a back support where the shell can be positioned off centre (and maybe even rotated to a degree) to accommodate the shape of the spine. Moving up to the top of the torso, where there is rotation around the shoulder girdle, rather than using a full shoulder harness, a single anterior strap to retract the shoulder on the forward rotated side may be all that is needed to help straighten up the torso (Figure 5).
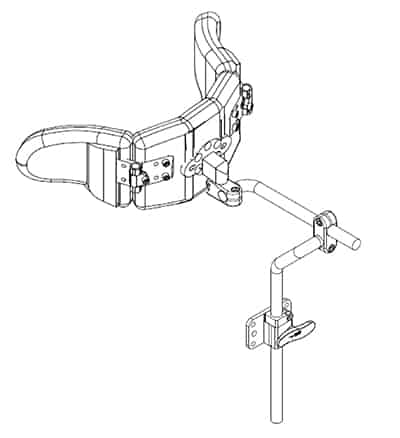
To accommodate asymmetry at the head, use a head support mounting system that allows off-centre positioning around the back of the occiput (for such a mounting system, see Figure 6). Use of a swing-away facial pad mounted to one side of the head rest can also help to position the head, but use your hands first (as with any pads) to find if the client has a tendency to move into a support or a tendency to move away from it (thereby using the client’s reflexes to guide you where to place the pads to achieve your mutual seating aims).
The Good, the Bad and the Ugly
Often a seating system is trying to work with an asymmetry that has arisen from the effects of gravity on the body, taking a small distortion and making it worse – the bad and the ugly. The clinician’s responsibility is to try to stop this happening in the first place, hence the obsession with symmetrical seating. (But, why do we still leave powerchair
joysticks at the end of the arm support, encouraging the client to end up leaning to that side, rather than using a swing away arm to allow a midline position when driving?)
Once an asymmetry has developed, then the assessment should consider whether anything can be first done to stop matters getting worse and then, second, seeing if the effects of time, habit and/or gravity can be reversed. It may have taken some years to reach where we are today and so it may also take some years to get back to where you want to be – or indeed it may never be possible so can only be accommodated.
However, there are places where asymmetry may be a good thing. Asymmetry often restricts our degrees of movement – the bad. But when we want to restrict movement, for example with a tendency towards not easily controllable athetoid movements, restricted movement is desirable – the good.
For these clients, creating asymmetries, such as crossing legs or hooking an arm around the back support uprights, can allow enough finer motor control elsewhere to be able to handle a joystick, for example. The seating system should allow this.
Finally, look at your position as you read this article. How symmetrically seated are you and how different is your position from ten minutes ago?
We spend a lot of time moving from one asymmetric posture to another for comfort, for communication, for functionality, for skin tissue health and so on. Are the wheelchairs we supply to our clients allowing them to move around as we do, while managing the good vs the bad of asymmetry?
References
- BS 8625:2019 Selection, placement and fixation of flexible postural support devices in seating London: BSI, 2019.
- https://thiis.co.uk/lets-get-it-cleartrunk-call-aligning-the-upper-body/

Further items can be found at www.beshealthcare.net. If you are interested in receiving further information on the topic, please contact barend@beshealthcare.net.
Dr Barend ter Haar has been involved in seating and mobility for over 30 years, including lecturing internationally and developing international seating standards.
Click to read more from the ‘Let’s get it clear’ series from Dr Barend ter Haar
https://thiis.co.uk/lets-get-it-clear-asymmetry-the-good-the-bad-and-the-ugly/https://thiis.co.uk/wp-content/uploads/2021/10/Fig-5.jpghttps://thiis.co.uk/wp-content/uploads/2021/10/Fig-5-150x150.jpgAnalysis & InsightsLet's Get It ClearNewsroomasymmetry,back supports,BES Healthcare,Dr Barend ter Haar,lateral support pad,Let's get it clear,wheelchair seating,wheelchair seating systemThe textbooks like to show us as sitting in symmetrical positions, but in reality, we are all asymmetrical and we spend most of our time sitting asymmetrically. This article reflects on the benefits vs challenges of asymmetry and how we might manage the asymmetries in setting up a wheelchair...Sarah SarsbySarah Sarsbysarah@thiis.co.ukEditorTHIIS Magazine